GENERAL
GENERAL
There are two types of radiofrequency (RF), conventional (CRF) and intermittent or pulsed radiofrequency (PRF).
In CRF, a continuous radiofrequency electric field (RFEF) is applied through an electrode to the active tip of a special needle and controlled heat is generated as a result of ion friction. When aimed at some target nerve, this heat (80-90°C) leads to nerve ablation and interruption of pain signals that are sent to the spinal cord and brain.
In PRF, the electric field is interrupted when temperature reaches 42°C and, as a consequence, the heat applied on the target nerve is non-ablative since it does not exceed 42°C. It has a rather neuromodulatory effect, reducing significantly pain signal conduction.
The radiofrequency electric field is produced by a special radiofrequency generator and applied to the target with a special needle that has an active non-insulated end. An electrode that is connected with the generator, is inserted through the needle. The generator has a screen with indications providing detailed information in the various parameters of the technique. (2,3,4,5)
INDICATIONS
Radiofrequency treatment is indicated for the treatment of nociceptive pain, as well as for some other types of neuropathic pain (with continuous and limited distribution) that are resistant to conservative treatment. This includes pain of unknown aetiology, such as the 12th rib syndrome or radicular pain that cannot be explained by any anatomic abnormality.
Neuropathic pain can be treated with radiofrequency if the nerve function remains at least partially intact, as for example in the cases of postoperative scar neuropathic pain, pressure-induced pain or pain due to nerve irritation. Pain induced by herniated intervertebral disc or peripheral neuropathy falls also within this category.
Radiofrequency treatment is not indicated when the pain is of central origin (impairment or disorder of the central nervous system, brain or spinal cord) or when there is severe psychopathology.
COMMON RADIOFREQUENCY TREATMENTS
• Conventional radiofrequency applied to the medial branch of the posterior ramus of the spinal nerve. This branch of the spinal nerve innervates the facet joints of the spine. These joints may cause chronic pain in the lower back or/and neck and more rarely in the chest due to degenerative changes, injury or poor positioning.
Conventional radiofrequency applied to the medial branch of the posterior ramus of the spinal nerve. This branch of the spinal nerve innervates the facet joints of the spine. These joints may cause chronic pain in the lower back or/and neck and more rarely in the chest due to degenerative changes, injury or poor positioning.
• Pulsed radiofrequency and more rarely conventional radiofrequency applied to the dorsal root ganglion (DRG) or to the part of the nerve that is the closest to the intervertebral foramen (if approaching DRG is not anatomically feasible). The treatment is indicated in radicular pain or radiculopathy from herniated intervertebral disc, radiculitis of unclear aetiology and the 12th rib syndrome. (2,4,6,7,29,32,33)
Pulsed radiofrequency and more rarely conventional radiofrequency applied to the dorsal root ganglion (DRG) or to the part of the nerve that is the closest to the intervertebral foramen (if approaching DRG is not anatomically feasible). The treatment is indicated in radicular pain or radiculopathy from herniated intervertebral disc, radiculitis of unclear aetiology and the 12th rib syndrome. (2,4,6,7,29,32,33)
• Intradiscal cooled radiofrequency. It is applied to treat chronic disc pain due to intradiscal degeneration, by ablating nociceptive receptors of the posterior part of the annulus fibrosus of the disc. These receptors produce pain signals that are interpreted by the brain as low back pain.
Intradiscal cooled radiofrequency. It is applied to treat chronic disc pain due to intradiscal degeneration, by ablating nociceptive receptors of the posterior part of the annulus fibrosus of the disc. These receptors produce pain signals that are interpreted by the brain as low back pain.
• Conventional radiofrequency in the sympathetic chain. The sympathetic chain is affected by many diseases, such as vascular insufficiency, pain of sympathetic aetiology, metastatic or osteoporotic fracture pain and discogenic pain due to intradiscal degeneration.
• Conventional radiofrequency in visceral nerves. It is highly effective in the treatment of visceral abdominal pain from malignant diseases involving the upper abdominal viscera (pancreas, liver, stomach etc) but also in some cases of benign pain (chronic pancretatitis, irritable bowel syndrome).(15)
• Pulsed radiofrequency in peripheral nerves. It is applied in cases of post-injury peripheral neuropathy. (1,9)
• Conventional or pulsed radiofrequency in the sphenopalatine ganglion. It is indicated in painful diseases resistant to conservative treatment, such as cluster headache and atypical prosopalgia. (16)
•  Conventional radiofrequency in the gasserian ganglion. Highly effective treatment for cases of trigeminal neuralgia that are resistant to conservative treatment.(10,11)
Conventional radiofrequency in the gasserian ganglion. Highly effective treatment for cases of trigeminal neuralgia that are resistant to conservative treatment.(10,11)
DESCRIPTION OF THE TECHNIQUE
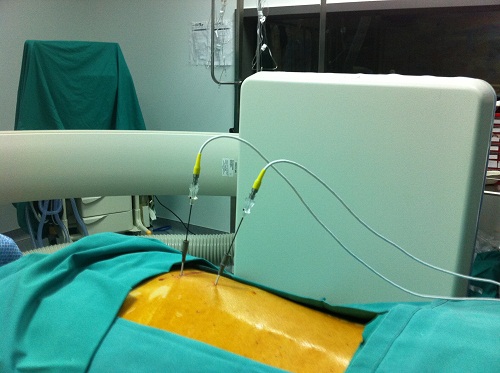
The technique is applied under local anaesthesia and fluoroscopic guidance. The patient does not need to be hospitalized and can go home a few hours after the intervention is completed. If considered necessary, light conscious sedation can be administered in order for the patient to be more relaxed and cooperative with the physician.
After following all antiseptic measures, a special needle is advanced to the target point with absolute accuracy and when the final proper site is confirmed with fluoroscopy from different views, an electrode that is connected with the radiofrequency generator is inserted through the needle.
Then follows sensory testing with nerve stimulation in order to bring the active tip of the needle as close as possible to the target. Once this is achieved, motor testing follows. The patient’s response to such a type of stimulation is observed in order to ensure that the active tip of the needle is within a safety distance from the motor nerve which is not the target.
Then, a local anaesthetic is administered and the electrode is heated with one of the two types of radiofrequency at the selected temperature for a few minutes and acts therapeutically. The rise of temperature is not painful for the patient because of the local anaesthesia provided.
RESULTS
Radiofrequency treatment is a safe and effective method for the treatment of several chronic pain syndromes. Should the pain be significantly reduced with the first radiofrequency application, the treatment can be applied repetitively. There is strong clinical evidence that radiofrequency treatment is effective in trigeminal neuralgia, radicular nerve pain and spinal pain Lord 2002). In a large study, 92,5% of patients with trigeminal neuralgia reported excellent or satisfactory relief after therapy of the trigeminal ganglion with conventional radiofrequency (Chen 2001).
Large randomized control studies (RCT) provide evidence for the denervation of facet joints in the lumbar and cervical spine with application of radiofrequency to the medial nerve branch. According to the latest review of the American Society of Interventional Pain Physicians (ASIPP) concerning interventional treatment of chronic spinal pain, facet joint denervation in the lumbar and cervical spine is a strongly evidence-based technique for a short period (3-6 months) and moderately evidence-based for a long period (> 1 year).
LITERATURE
- Letcher F, Goldring S. The effect of radiofrequency current and heat on peripheral nerve action in the cat. J Neurosurg 1968;29:42-7.
- Sluijter ME, Cosman ER, Rittman IIWB, et al. The effects of pulsed radiofrequency field applied to the dorsal root ganglion – a preliminary report. The Pain Clinic 1998;11:109-17.
- Cahana A, Vutskits L, Muller D. Acute differential modulation of synaptic transmission and cell survival during exposure to pulsed and continuous radiofrequency energy. J Pain 2003;4:197-202.
- Erdine S, Yucel A , Cunen A, et al. Effects of pulsed versus conventional radiofrequency current on rabbit dorsal root ganglion morphology. Eur J Pain 2005:9:251-6.
- Cosman ER Jr, Cosman ER Sr. Electric and thermal field effects in tissue around radiofrequency electrodes. Pain Med 2005;6:405-24.
- Higuchi Y, Nashold BS Jr, Sluijter M, et al. Exposure of the dorsal root ganglion in rats to pulsed radiofrequency currents activates dorsal horn lamina I and II neurons. Neurosurgery 2002;50:850-6.
- Van Zundert J, de Louw AJA, Joosten EAJ, et al. Pulsed and continuous radiofrequency current adjacent to the cervical dorsal root ganglion of the rat induces late cellular activity in the dorsal horn. Anesthesiology 2005;102:125-31.
- Sluijter M, Racz GB. Technical aspects of radiofrequency. Pain Practice 2002;2:195-200.
- Rohof OJJM. Radiofrequency treatment of peripheral nerves. Pain Practice 2002;2:257-60.
- Van Zundert J, Brabant S, Van de Kelft E, et al. Pulsed radiofrequency treatment of the Gasserian ganglion in patients with idiopathic trigeminal neuralgia. Pain 2003;104:449-52.
- Erdine S. Pulsed RF does not relieve trigeminal neuralgia. In: Raj PP ed. Proceedings of the 2nd World Congress of the World Institute of Pain; 2001, June 27-30; Istanbul, Turkey. Blackwell Science, 2001. p.384.
- Saal JA, Saal JS. Intradiscal electrothermal treatment for chronic discogenic low back pain: a prospective outcome study with minimum 1-year follow-up. Spine 2000;25:2622-7.
- Finch PM, Price LM, Drummond PD. Radiofrequency heating of painful annular disruptions: one-year outcomes. Spinal Disord Tech 2005;18:6-13.
- Teixeira A, Sluijter ME. Intradiscal high voltage, long duration pulsed radiofrequency for discogenic pain. A preliminary report. Pain Med (In press).
- Raj PP, Thomas J, Heavner J, et al. The development of a technique for radiofrequency lesioning of splanchnic nerves. Curr Rev Pain 1999:3:377-87.
- Sanders M, Zuurmond WW. Efficacy of sphenopalatine ganglion blockade in 66 patients suffering from cluster headache: a 12- to 70- month follow-up evaluation. J Neurosurg 1997;87:876-80.
- Sweet WH, Wepsic JG. Controlled thermocoagulation of trigeminal ganglion and rootlets for differential destruction of pain fibres. J Neurosurg 1974;40:143-56.
- Sluijter ME. Radiofrequency, part 2. Meggen, Switzerland. FlivoPress SA, 2003:159-166.
- Sluijter ME, Mehta M. Treatment of chronic back and neck pain by percutaneous thermal lesions. In: Lipton S, Miles J, eds. Persistent pain, modern methods of treatment. London, UK. Academic Press, 1981: Vol 3, 141-79.
- Sluijter ME. Radiofrequency, part 1. Meggen, Switzerland. FlivoPress SA, 2001:94-101.
- Gallagher J, Vadi PLP, Wesley JR. Radiofrequency facet joint denervation in the treatment of low back pain-a prospective controlled double-blind study in assess to efficacy. Pain Clinic 1994;7:193-8.
- van Kleef M, Barendse GA, Kessels A, et al. Randomized trial of radiofrequency lumbar facet denervation for chronic low back pain. Spine 1999;24:1937-42.
- Lord SM, Barnsley L, Wallis BJ, et al. Percutaneous radio-frequency neurotomy for chronic cervical zygapophyseal-joint pain. N Engl J Med 1996:335:1721-6.
- van Kleef M, Liem L, Lousberg R, et al. Radiofrequency lesion adjacent to the dorsal root ganglion for cervicobrachial pain: a prospective double-blind randomized study. Neurosurgery 1996;38:1127-31; discussion 1131-2.
- Dreyfuss P, Halbrook B, Pauza K, et al. Efficacy and validity of radiofrequency neurotomy for chronic lumbar zygapophysial joint pain. Spine 2000;25:1270-7.
- McDonald GJ, Lord SM, Bogduk N. Long-term follow-up of patients treated with cervical radiofrequency neurotomy for chronic neck pain. Neurosurgery. 1999;45:61-7
- van Suijlekom JA, van Kleef M, Barendse G, et al. Radiofrequency cervical zygapophyeal joint neurotomy for cervicogenic headache. A prospective study in 15 patients. Funct Neurol 1998;13:297-303.
- van Zundert J. Pulsed radiofrequency adjacent to the cervical dorsal root ganglion in chronic cervical radicular pain: a double-blind sham controlled randomized clinical trial. In: van Zundert, J. The use of pulsed radiofrequency in the treatment of chronic pain. (Thesis). Maastricht, the Netherlands. Datawyse, 2005.
- Munglani R. The longer term effect of pulsed radiofrequency for neuropathic pain. Pain 1999;80:437-9.
- Mikeladze G, Espinal R, Finnegan R, et al. Pulsed radiofrequency application in treatment of chronic zygapophyseal joint pain. Spine J 2003;3:360-2.
- Ahadian FM. Pulsed radiofrequency neurotomy: advances in pain medicine. Curr Pain Headache Rep 2004;8:34-40
- Van Zundert J, Lamé IE, de Louw A, et al. Percutaneous pulsed radiofrequency treatment of the cervical dorsal root ganglion in the treatment of chronic cervical pain syndromes: a clinical audit. Neuromodulation 2003;6:6-14.
- Teixeira A, Grandinson M, Sluijter ME. Pulsed radiofrequency for radicular pain due to a herniated intervertebral disc: an initial report. Pain Practice 2005;5:111-5.
- Houten JK, Errico TJ. Paraplegia after lumbosacral nerve root block: report of three cases. Spine J 2002;2:70-5.
- Cahana A, Macrea L, van Zundert J, et al. Pulsed radiofrequency: Current clinical and biological evidence available. Pain Med (In press).
- Pauza KJ, Howell S, Dreyfuss P, et al. A randomized, placebocontrolled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 2004;4:27-35.
- Koning HM, Koster HG, Niemeijer RF. Ischemic spinal cord lesion following percutaneous radiofrequency spinal rhizotomy. Pain 1991;45:161-6.
- Hsia AW, Isaac K, Katz JS. Cauda equina syndrome from intradiscal electrothermal therapy. Neurology 2000;55:320.